| Medulla Oblongata | |||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
The medulla relays sensory information to thalamus and contains major regulatory centers in its reticular formation
|
|||||||||||||||||||||||||||||
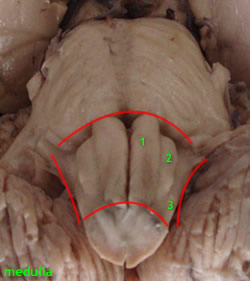
| The internal anatomy of the closed and open medulla demonstrates the following structures .
|
|||||||||||||||||||||||||||||
| Fiber bundles | |||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
Blood supply to the medulla oblongata |
|||||||||||||||||||||||||||||
Four main arteries supply the medulla oblangata • Anterior spinal arteries supplying the antero-medial structures namely - Pyramids - Medial lemniscus - Hypoglossal nucleus - Medial Longitudinal fasciculus - Solitary and vagal nuclei • Posterior spinal arteries supplying the fasciculus and nucleus gracilis and cuneatus • Posterior inferior cerebellar artery supplying the retro-olivary region, including - Spinothalamic tract - Spinal trigeminal nucleus - Nucleus ambiguus Hypothalamo spinal tracts • Bulbar branches of the vertebral artery supplying the pyramids, hypoglossal, nucleus, and inferior olivary nuclear complex.
|
|||||||||||||||||||||||||||||
| Tracts of the Medulla Oblangata
The medulla oblangata contains all the tracts ascending to the brain, and those descending to the spinal cord. Key among them are
|
|||||||||||||||||||||||||||||
| Applied anatomy | |||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||