| The
Cavernous Venous Sinus |
|
| This is clinically
very important on account of the following:
- It's numerous extracranial
and intracranial communications.
- The structures contained within
it and its walls.
- Its proximity to the pituitary
gland.
|
| |
|
| Location |
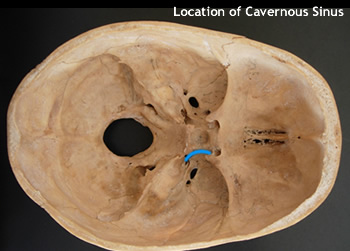 |
- It is found on each side of the sella turcica and
the sphenoid body.
- Extending from the superior orbital fissure to the
apex of the petrous temporal bone.
- The cavum trigerminale is located lateral to it.
|
| |
|
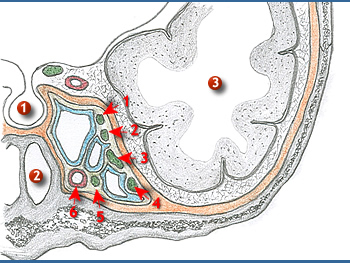
| Relations
|
|
Medially:
Pituitary gland(1) and sphenoidal air cells(2).
Superiorly:
Temporal lobe of the brain(3).
Laterally:
Trigerminal ganglion and nerve.
Anteriorly:
The contents of the superior orbital fissure and ................the optic nerve.
Posteriorly:
Petrous temporal bone.
Within:
Lateral wall - Oculomotor, trochlear, ophthalmic and ...........maxillary nerves.
In
it: Carotid siphon with its associated sympathetic
plexus, ........the abducens nerve and venous blood. |
| |
|
| Inter-cranial
communications |
 |
- Superficial middle cerebral vein.
- Intercavernous sinuses connect the two sides.
- Sphenoparietal sinus.
- Superior petrosal sinus connects it to the transverse
sinus or sigmoid.
- Inferior petrosal sinuses connect it to the internal
jugular vein.
|
| |
|
| Extracranial communications |
- Superior and inferior ophthalmic veins.
- The pterygoid venous plexus Via emissary veins.
- The pharyngeal venous plexus.
Note that the facial vein communicates through the ophthalmic
veins and the pterygoid plexus. |
| |
|
| Clinical
correlates on the cavernous venous sinus |
| Spread
of infections |
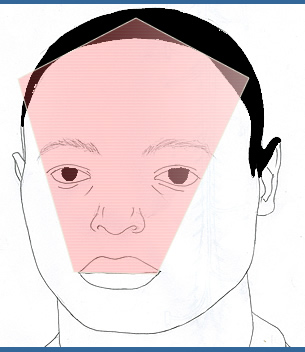 |
Danger area of the face
 Infections from here spread to cavernous sinus via opthalmic veins
Infections from here spread to cavernous sinus via opthalmic veins
|
| |
|
Cavernous
sinus thrombosis |
| A
common effect of infection of in a venous sinus is thrombosis.
The risk is higher in the cavernous sinus due to the slow movement of
blood. The effects are usually:
- Back-flow into the connecting
veins, for example ophthalmic veins leading to exopthalmos
and engorged conjuctiva (chemosis)
- Compression of the nerves to
the extraocular muscles leading to ophthalmoplegia
and impaired sensation in the area of supply of Cranial
V1 and V2.
|
| |
|
| Arteriovenous
fistula |
| This
may be produced by fractures of the bases of the skull, in which the
internal carotid artery tears within the cavernous sinus. Arterial blood
rushes in to the sinus, enlarging it and forcing blood out of it through
the communicating veins. This causes exophthalmos
and chemosis
on the side of the injury. In these circumstances, the bulging
eye pulses in synchrony with the radial (or any other) pulse.
This condition is called pulsatile exophthalmos.
|
| |
|
| Others |
| Infections
spreading to the sinuses may affect the pituitary and the many cavernous
sinus communications may provide alternative routes for spread of malignancies. |
| |
|